At this year’s EASD conference, one of the most interesting topics was the future of type 1 diabetes treatment. The spotlight was on GLP-1 receptor agonists and GIP-based therapies. While insulin remains the irreplaceable foundation of therapy, it is becoming increasingly clear that insulin alone is often not enough.
Even with the most advanced insulin pumps, sensors, algorithms, and available technology, many people with type 1 diabetes still struggle with major glucose fluctuations, weight gain, and the risk of complications. The reason is that type 1 diabetes is not caused only by a lack of insulin. At its core, it involves a whole range of complex metabolic disturbances.
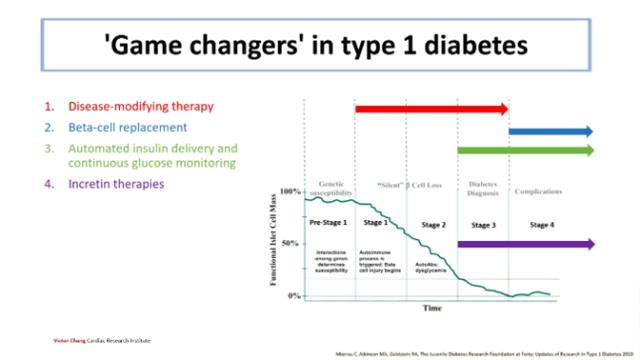
“Game Changers” in Type 1 Diabetes
Besides insulin itself, which remains the greatest “game changer” in the history of diabetes, progress in pharmacology and technology has brought a number of new possibilities that can significantly improve disease management.
Experts highlighted four areas that already have, or may soon have, the potential to completely change the way type 1 diabetes is treated:
1. Disease-modifying therapies – treatments aimed at the autoimmune process and preservation of beta cells.
2. Beta-cell replacement – restoration or transplantation of beta cells in the pancreas.
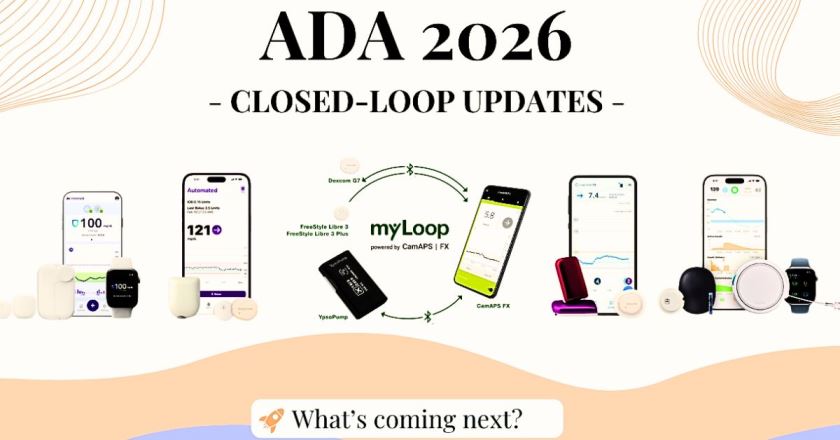
3. Automated insulin delivery and continuous glucose monitoring – technologies that are already transforming everyday life for people with diabetes.
4. Incretin-based therapies – a new group of medicines, including GLP-1 and GIP agonists, which are being increasingly studied as an addition to insulin therapy.
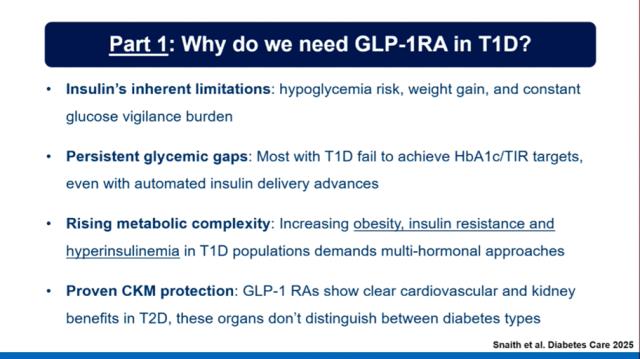
Why GLP-1 in Type 1 Diabetes?
Incretins, especially GLP-1 receptor agonists, have already proven effective in type 2 diabetes and obesity treatment. They stimulate insulin secretion, reduce glucagon, slow gastric emptying, and decrease appetite.
At EASD, the key question was: could these same mechanisms also benefit people with type 1 diabetes?
The answer may be yes, because in type 1 diabetes GLP-1 receptor agonists could potentially:
- reduce the risk of hypoglycemia,
- increase time spent in the target glucose range,
- support weight loss,
- and have favorable effects on cardiovascular health.
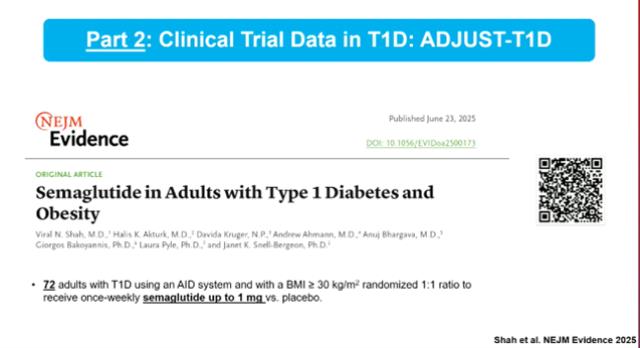
What Do the Studies Show?
The first evidence is already available. Clinical studies such as ADJUST-T1D have shown encouraging results for semaglutide, best known under the brand names Ozempic® and Wegovy®.
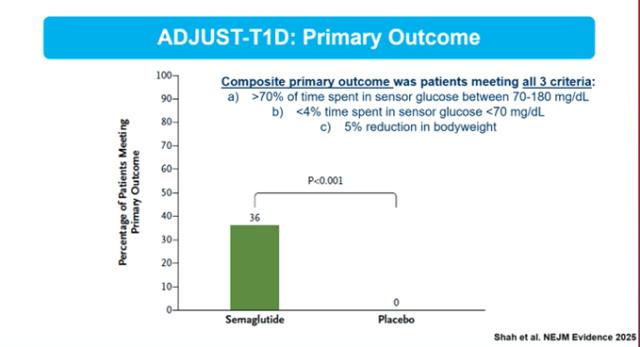
- More than one third of participants achieved a composite treatment goal: better glucose control, fewer hypoglycemic episodes, and weight loss.
- Total insulin requirements were reduced by up to 40%.
- Time in range significantly improved.
These results suggest that GLP-1 receptor agonists could become a valuable ally in the treatment of type 1 diabetes, especially for people who also struggle with obesity and insulin resistance.
GIP and GLP-1 – A New Combination
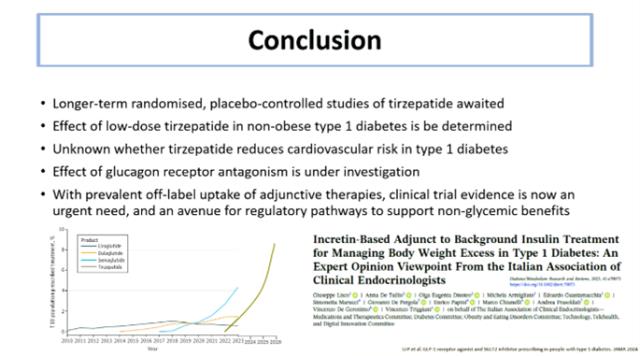
In addition to GLP-1, increasing attention is also being given to GIP, another incretin hormone that affects fat tissue and lipid metabolism. Combining both pathways has led to the development of tirzepatide, marketed as Mounjaro®, which has shown even stronger metabolic effects.
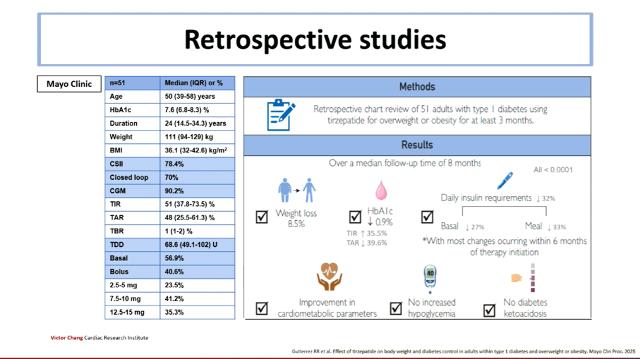
Retrospective studies, including one conducted at the Mayo Clinic, have shown:
- average weight loss of 8 to 10%,
- a significant reduction in HbA1c,
- a reduction in daily insulin doses by about one third,
- and no increase in the risk of ketoacidosis or severe hypoglycemia.
These findings suggest that the combination of GLP-1 and GIP-based therapy could represent the next major step in type 1 diabetes treatment. However, longer-term randomized studies are still needed before firm conclusions can be made.
Key Conclusions from the Lecture
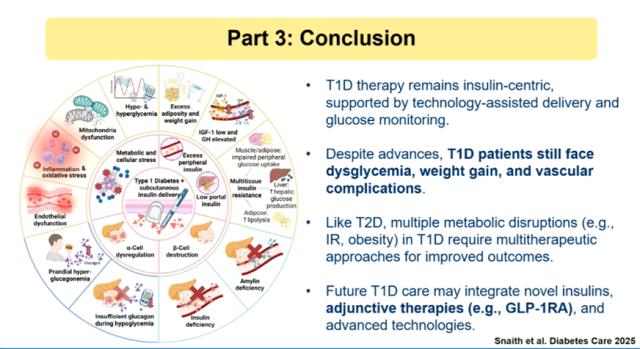
The main message from the experts was clear: although insulin remains the fundamental therapy for type 1 diabetes, it is not enough on its own. Patients continue to face dysglycemia, obesity, and complications, which is why the future is moving toward a multi-therapy approach.
This means that in the coming years, insulin may increasingly be complemented by new medicines such as GLP-1 receptor agonists, GIP-based therapies, and tirzepatide, as well as by advanced technologies and treatments that target the disease process itself and aim to preserve beta-cell function.
In other words, the “game changers” in type 1 diabetes will not be a single medicine or a single device. They will be a combination of different innovations that, together, could significantly improve quality of life and treatment outcomes.
If this topic interests you, we also invite you to read our article: “Check-ups with Your Diabetologist – Why They Matter Specifically to YOU.”
Author: Antonia Precali